What is the Difference Between Biest vs Estradiol?
Estradiol and biest are used typically for hormone replacement. They are both forms of estrogen and used for symptoms of low estrogen. Commonly they are used for menopause. The average age of menopause is 51.5 years old, although symptoms could start as early as the 40’s. The gradual decline of ovarian function can cause symptoms in which estrogen is helpful. In surgical-menopause, the uterus and ovaries are removed, is a different story. When the ovaries are removed, instantly puts a woman into menopause. In menopause, there is a decline of the sex hormones over time. But in surgical menopause, a woman goes from having a good amount of sex hormones to having none. This instant transition can cause instant intense menopausal/low estrogen symptoms.
Estrogen is also good for bone density. Incorporating diet, lifestyle, and supplementation with estrogen can help preserve and improve bone density. After removal of the uterus and ovaries (surgical menopause), it can be beneficial to provide estrogen hormone therapy to protect bone density. Especially if the surgical removal of the ovaries happens to a younger female such as the 30’s.
Estrogen and hormone replacement are also used for libido, skin integrity, anti-aging, cognition, sleep, hot flashes, night sweats and vaginal atrophy. Estrogen hormone replacement can be helpful. But deciding on what type, dose, the vehicle of administration for an individual can be a bit more challenging. Estrogen hormone replacement therapy is not “one dose fits all.”
It needs to be tailored to that particular female depending on her goals, personal and family history and especially if she has a uterus. You do not want to do any kind of estrogen hormone replacement without progesterone if a female has a uterus. Estrogen replacement alone without progesterone can put a woman at risk for uterine cancer and spotting or bleeding. Progesterone (bioidentical) is helpful for the body in many ways, but that is for another post.
First I would like to start off by explaining what estradiol and Biest are:
What is Estradiol?
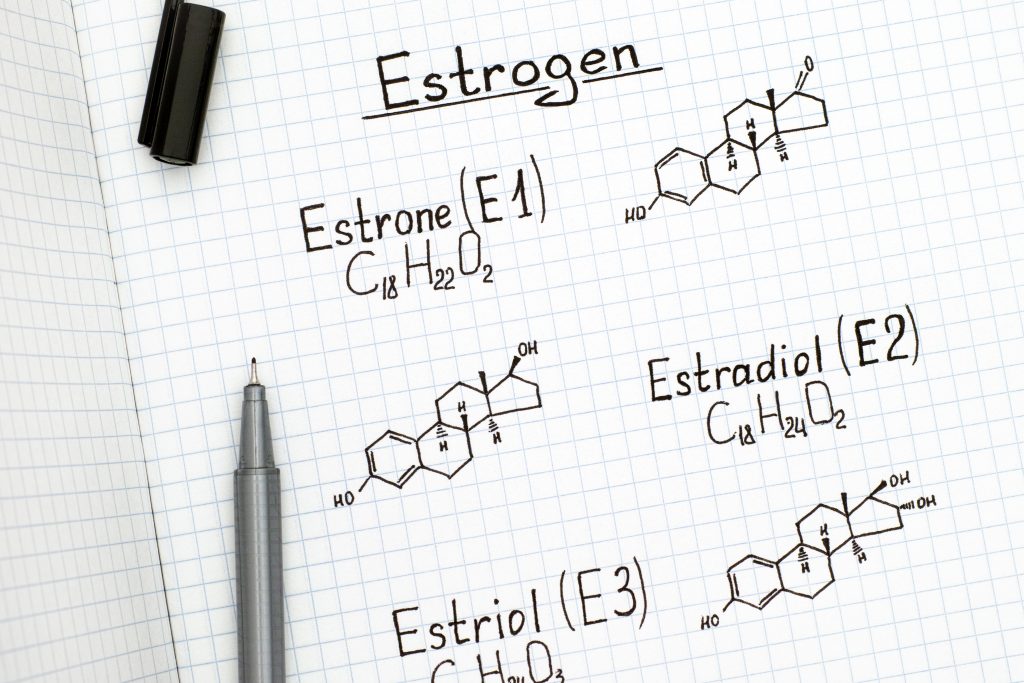
We make three estrogens in our bodies. Those are estrone, estradiol, and estriol.
- Estrone: Estrone is an undesirable estrogen. We tend to make more of it as teens that have just started their periods. Estrone is also made by our fat tissues. Having too much estrone can cause unwanted symptoms such as irritability, moodiness, increase appetite/cravings for sugar, easy weight gain.
- Estradiol: Estradiol is the strongest of the three estrogens. Estradiol is helpful for maintaining and building bone density. Estradiol is good for the cardiovascular system. It can help raise HDL (high-density lipoproteins), which is the desirable/”good” cholesterol. Estradiol is great for the brain and memory recall. In menopause, one main symptom is low memory recall. Many women report they will forget what they were saying mid-sentence. If asked a question, it feels like the answer is in there, but won’t come out. Blurting out the answer 2-15 minutes later. Low levels of estradiol in menopause is what causes the hot flashes and night sweats. Estradiol is also involved in female libido. Estradiol is what runs the ship for female sex drive. It is commonly thought that testosterone is for sex drive. Testosterone can be excellent for male libido, but it only has a slight effect on women. Honestly, for us ladies, it is about the estradiol when it comes to sex drive, thinking about and initiating sex.
- Estriol: is the weakest or most gentle of the estrogens. Estriol is helpful for skin and mucous membranes. Estradiol is conventionally used to treat vaginal atrophy. But I find estriol is much better for vaginal dryness and pain with intercourse from atrophy. Estriol is the unsung hero when it comes to the estrogens as it can help balance estradiol.
As mentioned above, estradiol is quite strong. Sometimes estradiol can take over the entire hormonal show. Causing uterine bleeding, moodiness, weight gain, tender swollen breasts and trouble sleeping. Estriol is excellent to rein in and balance the negative effects of estradiol. I have also found estriol to be helpful for urinary incontinence. The urethra can become lax when estrogen levels drop. This can cause urine leaking with coughing, laughing, exercise. Or when it is time to go, hurry up and find a bathroom because there is no leeway.
Back to Estradiol:
Estradiol treatment for low estrogen levels is a bioidentical form of hormone replacement (BHRT). Estradiol hormone replacement comes in many forms.
- Oral: Oral estradiol used to be popular in the early 2000’s and is still used occasionally today. Oral estradiol can be appropriate for the particular individual. But can be hard on the liver and can create estrogen metabolites such as 2OH estrone and 4OH estrone which in high levels are not healthy to the body. If oral estradiol is appropriate for a particular female, then close observation of the liver enzymes and estrogen metabolites are necessary.
- Patch: Estradiol patches are currently very common for estradiol bioidentical hormone replacement. Patches come in different dosing and are applied twice weekly. Patches are easy to use as you just slap it on twice a week. The drawback is the estradiol levels tend to be quite high after first application and then dwindle fast over the next 2-3 days. Some women complain or the patch getting dirty, falling off and wary of swimming or taking baths because it will fall off. While it is easy to apply, it is hard to finesse the perfect balance of BHRT. There are only three doses available making it more like a one size fits all.
- Creams/gels: These are similar to patches, they are transdermal, and the estradiol will go through the skin into the bloodstream. Transdermal estradiol is not hard on the liver like oral forms of estradiol are. Although they usually need to be applied once to twice a day, compliance can be an issue. Also, care is needed to make sure that the cream is applied to a part of the body that will not transfer to others. Usually, the inner thigh is a great place to apply the cream, so it doesn’t get on other people, kids or animals.
- Pellets: Pellets came out in the early 2000’s and got popular around 2008-2014. But due to side effects, cost and invasiveness of the procedure it’s not as popular currently. Pellets are commonly replaced every three months (some people will try to stretch that longer). But getting them replaced every three months can be costly, usually around 400-600$. Also, it can be an invasive procedure of minor surgery to insert the pellet in the gluteal muscle. Once the pellet is in, you do not have to worry about taking hormones as the pellet releases the hormone on its own. The drawback is, once inserted you cannot adjust the dose. So if the level of estradiol is high and there are side effects. There is not much to be done except wait.
- Sublingual troches: These estradiol forms come in little solid squares. You put them under your tongue or in the cheek of your mouth, and it dissolves. This allows it to be absorbed through the mucous membranes of the mouth. While sublingual is better absorbed, a lot can end up getting swallowed. Then it goes through the digestion, putting a burden on the liver. Others complain that the troches take a long time to dissolve and do not taste very good. They are used once to twice daily.
What is Biest?
You will not find Biest dispensed by a big-box pharmacy and it is not usually prescribed by your conventional doctor. That is because biest is a combination of estradiol and estriol. Estriol is not available commercially but is dispensed through compounding pharmacies.
As I mentioned above, estriol is the gentlest, weakest form of estrogen. Estriol can help balance the negative effects of estradiol. Estradiol is a great hormone but is super strong. If you combine estriol with estradiol, it can blunt the negative effects of estradiol.
Those symptoms of estradiol alone being, moodiness, weight gain, anxiety, puffiness, water weight, acne, tender breasts, spotting/bleeding, carb cravings/increased appetite. If estriol is combined with estradiol, that can minimize the negative symptoms, while promoting the positive. Those positive benefits are, reducing hot flashes/night sweats, increasing libido, improving vaginal atrophy, improving brain fog, metabolism to name a few.
The trouble with biest is not many doctors know how to dose it. If a woman has been on conventional HRT, especially Premarin/Prempro, taking biest will do nothing for them. Conventional, synthetic or non-bioidentical hormone therapy is very strong and puts a huge burden on the liver. Taking biest to replace these harsh medications is like taking nothing. I’ve had patients come to see me, scoffing at biest because “it doesn’t work!”. Biest is a gentle, very safe form of BHRT. There is a big difference between giving someone that has never been on BHRT, biest compared to someone that was on an estradiol patch or Premarin. This is where the dosage of the estradiol and estriol is extremely important.
Forms of Biest:
Biest comes in almost as many forms as estradiol.
- Creams: Transdermal creams of biest are the most common form dispensed. It is usually applied once to twice a day. As mentioned above there needs to be care not to get it on other members of the family or pets. Applying to the inner thigh will ensure that it doesn’t get on anyone else. Biest can also be applied vaginally, but this is not common. As if you apply biest to the vaginal mucous membranes the longevity in the bloodstream is shortened. Estriol is more commonly applied to the vaginal mucous membranes for atrophy.
- Suppositories: Occasionally you will see a vaginal suppository of biest. Usually, vaginal suppositories consist of estriol only to help with vaginal atrophy and urinary incontinence.
- Sublingual troches: As mentioned above sublingual administration bypasses the digestion, but there still is a likelihood of it ending up being swallowed. With compounding pharmacies, you can get some with flavoring added, such as orange or mint. This helps the taste become more tolerable.
- Pellets: Biest can be used in pellets for BHRT. But again the dosage cannot be adjusted after inserting the pellet. And it is still invasive and can be on the pricey side for the procedure. Some people do like the ease of the pellets. But if a female has a uterus, it is important to take an oral form of progesterone on top of the insertion of the pellet. This is to protect the uterus from the risk of uterine cancer and from bleeding and spotting.
- Patches: Biest is not dispensed as a topical patch. But that could change in the future.
I would like to quickly interject the topic of progesterone. This blog is about the differences between estradiol and biest. Whether you are taking estradiol or biest, in most cases it is important to incorporate progesterone. This is important for the safety as well as achieving the BHRT goals of the patient. Progesterone uses, forms, dosages and BHRT goals are another long-ish post. I know you readers are smart and likely more educated on bioidentical hormones than most doctors. So I would be amiss if I didn’t point out progesterone is important in BHRT, but I am going to leave that for another blog.
Dosages and ratios:
This is where the tricky part comes in for BHRT. Whether you are using estradiol or biest, the real art is in the dosage. As I mentioned earlier, estradiol can be quite strong. With estradiol you want to try and keep the dose as low as possible, yet still enough for the BHRT goals. But with biest, you have so much more versatility with the dosage.
Biest is a combination of estriol and estradiol. The most common ratio of biest is 80:20. Meaning 80% of the dose is estriol, and 20% is estradiol. For example, 5mg of biest would contain 4mg of estriol with 1mg of estradiol. But with compounding, you can do any ratio that would feel that patient’s needs. Sometimes the typical 80:20 ratio is not appropriate for a particular patient. I think it is easier to use examples to explain the many options you can have with biest.
Patient 1: “Grace” came to see me, frantically worried. Her gynecologist was unwilling to prescribe her Premarin anymore. The second she stopped it, she felt terrible. Frequent intense hot flashes and night sweats. She could not sleep at all, and her mood was terrible. I mentioned using a bioidentical form, biest. She immediately blew that off with a laugh and said her gynecologist tried that and it didn’t help one bit. It turned out she was on an 80:20 ratio dose of biest and was only taking it in the morning. This is where the magic of dosing for the individual is awesome.
The dose that Grace had taken was so low, that is was basically a glorified moisturizer for her. What she needed and had success with was a ratio of 50:50 and taken twice a day. It was an even dosage between the estriol and estradiol. Grace needed the extra estradiol to bridge the gap from Premarin to bioidentical hormones. Premarin is strong, and it puts a burden on the liver. I just needed to increase the estradiol and work on her liver processing to start. That immediately took care of her symptoms. With time, I was able to reduce her dosage and change the ratio of estriol to the estradiol.
Patient 2: “Maggie” came in distraught, saying she had tried biest and it didn’t work for her. When she had taken the biest, she gained 8 lbs, and her breasts grew huge and were tender. She is 51 years and started bleeding and having periods again. It turned out for Maggie that her progesterone was too low. Plus the 80:20 ratio of biest was too strong for her. I switched her to a progesterone capsule to protect the uterine lining. And I reduced her biest and changed it to a 90:10 ratio.
Patient 3: “Samantha” came to see me for her menopausal symptoms. She was having about 4 moderate hot flashes during the day. She said the day flashing was not that bad and tolerable. But nighttime was another story. At night she would have three really intense night sweats. She would sleep on a beach towel and have to change her PJs at night. Then it would take “ages” to get back to sleep. Samantha was getting calf and feet cramps because she was sweating so bad, it made her dehydrated. Samantha had never taken hormones or “anything like this stuff” before.
I put her on a basic 80:20 ratio of a low dose biest twice a day. The dose that worked for her was a small dose in the morning and a higher dose at night. It took care of her menopausal symptoms and Samantha was able to get a good night’s sleep. Honestly, Samantha was easy. She had never taken hormones like Grace had. And she was not super sensitive to them like Maggie. I think that is where biest get a “bad name”. From their personal history to their family history, everyone is uniquely different. What works for one woman is not going to work with another. Like I said, dosing and prescribing BHRT is an art. One size will never fit all.
I would like to summarize the difference between estradiol and biest. Biest is a combination of estriol and estradiol. Biest can have any ratio of estriol to estradiol depending on the goals, symptoms, and safety of the patient.
Estradiol is the strongest form of the estrogens. In many cases using estradiol alone can be too strong for the patient resulting in symptoms of excess estrogen. A particular estradiol dose might be perfect for controlling the hot flashes of a patient, but also causing weight gain and moodiness. When you reduce the dose of estradiol the moodiness and weight gain subside, but they are back to hot flashing again. That is where using biest would be helpful.
The estriol in biest can help balance some of the negative effects of estradiol, while at the same time able to resolve symptoms of low estrogen. Having the versatility of the different dosing and ratios of biest can also help women wean off hormones if they cannot take them anymore. The difference is the option of using estriol mixed with the estradiol. It can give so much more variability of dosing based on an individual’s BHRT goals.
Hopefully, this article gave you a better idea of the differences between Biest and Estradiol. If you have any questions, please leave a comment below or send an email to [email protected].
